-Annette J. Bouwhuis-Van Keulen, Jurrijn Koelen, Liesbeth Eurelings-
Bontekoe, Christien Hoekstra-Oomen & Gerrit Glas
-To cite this article: Annette J. Bouwhuis-Van Keulen, Jurrijn Koelen, Liesbeth Eurelings-
Bontekoe, Christien Hoekstra-Oomen & Gerrit Glas (24 Aug 2023): The evaluation of religious
and spirituality-based therapy compared to standard treatment in mental health care:
-A.multi-level meta-analysis of randomized controlled trials, Psychotherapy Research, DOI:
10.1080/10503307.2023.2241626
-To link to this article: https://doi.org/10.1080/10503307.2023.2241626https://doi.org/10.1080/10503307.2023.2241626
-ANNETTE J. BOUWHUIS-VAN KEULEN1∗, JURRIJN KOELEN2∗,
LIESBETH EURELINGS-BONTEKOE3, CHRISTIEN HOEKSTRA-OOMEN4, &
GERRIT GLAS1
-1Faculty of Humanities, Department of Philosophy, VUmc Amsterdam, Amsterdam, The Netherlands; 2Faculty of
-Behavioural, Management and Social Sciences, Department of Psychology, Health and Technology, University of Twente,
-Enschede, The Netherlands; 3Faculty Social Sciences, Department of Clinical Psychology, University of Leiden, Leiden, The
-Netherlands & 4Psychology Practice Edelweis, Delft, The Netherlands
(Received 1 December 2022; revised 20 July 2023; accepted 21 July 2023)
.ABSTRACT.
-Objective Psychotherapies are increasingly incorporating spiritual and religious systems of belief and practice, which aligns
-with recent developments toward person-centered treatments. The main objective of this meta-analysis was to compare the
-efficacy of a religion and spiritually-based (R/S) therapy to non-R/S treatments.
-Method A multi-level meta-analysis was conducted to compare randomized controlled studies of the efficacy between R/Sbased
-and regular treatments in mental health care setting. Inclusion criteria were diagnosis, psychotherapeutic treatment,
-and explicitly religion/spirituality therapy. Outcome was assessed for symptoms and for functioning separately, and
-combined. We also examined several moderators, such as type of comparison, outcome domain, and diagnosis.
-Results Overall effect sizes obtained from 23 studies and 27 comparison groups indicated that a R/S treatment is moderately
-more efficacious compared to regular treatments at posttreatment (g = .52, p < .01) and at follow-up (g = .72, p < .01) (only
-available for symptoms). Results were similar for symptoms (g = .44, p < .01) and functioning (g = .62, p < .01).
-Conclusion In patients with a strong religious and spiritual affiliation, treatments with a focus on religious and spiritual
-issues are more efficacious than non-R/S-based therapy. Limitations as well as future directions are discussed.
-Keywords: meta-analysis; randomized controlled trials; religious and spirituality-based therapy; mental health care; psychotherapy
-Clinical or methodological significance of this article: This meta-analysis expands knowledge about R/S-based
-psychotherapy and clarifies inconsistent findings from previous meta-analyses. Person-centered therapy with attention to religious and spiritual language, questions, and subjects are efficacious, especially for depressed patients.
:چکیده-
رواندرمانیهای عینی به طور فزایندهای سیستمهای معنوی و مذهبی باور و عمل را در بر میگیرند، که با پیشرفتهای اخیر در جهت درمانهای فردمحور همسو است. هدف اصلی این متاآنالیز، مقایسه اثربخشی درمان مبتنی بر مذهب و معنویت (R/S) با درمانهای غیر R/S بود.
روش: یک متاآنالیز چند سطحی برای مقایسه مطالعات تصادفی کنترلشده از اثربخشی بین درمانهای مبتنی بر مذهب و معنویت و درمانهای معمول در محیط مراقبتهای سلامت روان انجام شد. معیارهای ورود شامل تشخیص، درمان رواندرمانی و درمان صریح مذهبی/معنویت بود. پیامد برای علائم و برای عملکرد به صورت جداگانه و ترکیبی ارزیابی شد. ما همچنین چندین تعدیلکننده، مانند نوع مقایسه، دامنه پیامد و تشخیص را بررسی کردیم. -نتایج اندازههای اثر کلی بهدستآمده از ۲۳ مطالعه و ۲۷ گروه مقایسه نشان داد که درمان R/S در مقایسه با درمانهای معمول در پسدرمان (g = 0.52، p < 0.01) و در پیگیری (g = 0.72، p < 0.01) (فقط برای علائم موجود است) نسبتاً مؤثرتر است. نتایج برای علائم (g = 0.44، p < 0.01) و عملکرد (g = 0.62، p < 0.01) مشابه بود.
-نتیجهگیری در بیمارانی که وابستگی مذهبی و معنوی قوی دارند، درمانهایی با تمرکز بر مسائل مذهبی و معنوی مؤثرتر از درمانهای غیرمبتنی بر R/S هستند. محدودیتها و همچنین مسیرهای آینده مورد بحث قرار گرفتهاند.
-کلمات کلیدی: متاآنالیز؛ کارآزماییهای تصادفی کنترلشده؛ درمان مبتنی بر مذهب و معنویت؛ مراقبتهای سلامت روان؛ رواندرمانی
- اهمیت بالینی یا روششناختی این مقاله: این متاآنالیز دانش در مورد رواندرمانی مبتنی بر را گسترش میدهد و یافتههای متناقض از متاآنالیزهای قبلی را روشن میکند. درمان متمرکز بر فرد با توجه به زبان، سوالات و موضوعات مذهبی و معنوی، به ویژه برای بیماران افسرده مؤثر است.
.Introduction.
-The Pew Research Centre (2015) estimates that in 2050 86.8% of the 9.3 billion world population will have a religious/spiritual affiliation.
-Each religious tradition has its own worldview and perspective on human beings, and teaches its followers how to live life in accordance with spiritual values.
-Religious knowledge, experiences and activities influence mental health and psychopathology (Stulp et al.,2019), personality (Schaap-Jonker et al., 2017), and coping strategies (Pargament, 2007).
-Therefore religious and spiritual affiliations in the domain of mental health care should be considered important, which is consistent with person-centered approaches (see e.g., Glas, 2019, 2021).
-Since the end of the last century, attention for the existential dimension of being human and suffering, and thus patients’ religious or spiritual world views, has notably increased in clinical treatment (Glas,
2021; van Os et al., 2019).
-The American PsychologicalAssociation (APA) has developed guidelines for dealing with cultural, religious, and spiritual issues in treatment (APA, 2017).
-Moreover, scientific research has revealed the importance of spirituality to the clinical process, such as the protective effect of spirituality on mental health (Stulp et al., 2019), as well as the influence of religious coping strategies on psychopathology (Ano & Vasconcelles, 2005).
-As part of these developments, integrative religious and spiritual treatment approaches have been developed that endorse an active search for the sacred, and how this reflects on a person’s coping with mental illness (Pargament, 2007; Richards & Bergin, 2005).
-These religious/spiritual treatments use vocabulary not used in regular psychotherapy, and they tend to strongly emphasize the mobilization of hope, acceptance, and forgiveness, amongst other concepts.
-In this more holistic context, with attention to existential, transcendent, and meaning-making questions, mental disorders are treated and patients are met (Glas, 2021).
-In this contribution, we focus on psychotherapeutic treatments that seek to improve the psychological
well-being of patients, by using religious or spiritual sources related to a transcendent dimension and a
search for the sacred. Following Worthington et al. (2011), we use the term religious and spiritual based (R/S) therapy to refer to these treatments, although other terms are also used, such as spiritually integrated psychotherapy (Pargament, 2007), faith adapted therapy (Anderson et al., 2015), body–mind-spirit therapy (Hsiao et al., 2011), religion accommodative psychotherapy (Paukert et al., 2011).
-Mindfulness-based treatments are not included because these interventions do not focus on finding meaning in the transcendent dimension, but rather at promoting non-judging attention toward mental states in the current moment, independently of religious or spiritual content.
-Our main aim is to address the question of whether R/S treatment is more efficacious than non-R/S treatments for patients suffering from mental disorder.
.Previous Meta-Analyses on the Effectiveness of R/S Treatments.
-In recent years, several meta-analyses have been published on the effectiveness of R/S treatments compared to non-R/S treatments or no treatment (Anderson et al., 2015; Captari et al., 2018; McCullough, 1999; Smith et al., 2007; Worthington et al., 2011).
-Results are somewhat inconsistent, probably due to the choices of inclusion criteria used, variations in statistical methods, treatment criteria, and control groups.
-Two meta-analyses focused only on randomized controlled trials (Anderson et al., 2015; McCullough, 1999), two studies included also quasi-experimental studies (Captari et al., 2018; Worthington et al., 2011) and in the metaanalysis of Smith et al. (2007) single-group pre- to posttest designs were also allowed.
-Due to the diversity of research methods, a considerable variation in the quality of the included studies was indicated (Anderson et al., 2015; Paukert et al., 2011), which may affect the results. Second, the meta analyses apply different inclusion criteria in terms of diagnosis and treatment. McCullough (1999) includes all psychological diagnosis, while Anderson et al. (2015) is limited to depression and anxiety disorders, and the remaining three meta-analyses aggregate both psychological, psychosocial, and physiological diseases.
-In addition, four meta-analyses use a broad definition of psychotherapy, allowing for much variation in treatments (for example one session therapy, internet therapy, lifestyle training, and prayer groups).
-Finally, the inconsistent results are possibly due to the variation in treatment and control groups.
-Table I shows the results of the published meta-analysis split by, essentially, three comparing groups.
-The first comparing group, the blended group, was used in the meta-analysis of Captari et al. (2018), McCullough (1999) and Worthington et al. (2011) and compared a regular therapy with religion accommodative regular therapy, using equal amounts of treatment as inclusion criteria.
-Mainstream treatment (i.e. cognitive behavioral therapy, (CBT)) was adapted from a religious mindset, appropriate within the psychological theory (i.e. Religious Cognitive Behavioral therapy (RCBT)).
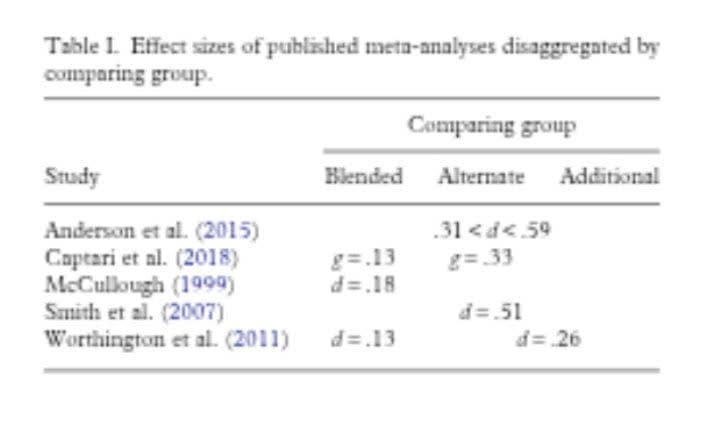
-They found an effect size of, respectively g = .13, d = .18 and d = .13, indicating that R/S therapy is slightly more effective than regular therapy. Secondly, Captari et al. (2018) compared a R/S treatment with a standard therapy, with both treatments having a completely separate theoretical background (i.e. Spiritual Integrated treatment compared to Rational Emotive Therapy).
-They found for this comparison with a so-called alternate treatment group an effect size of Hedges’ g.33, in favor of the R/S therapy. Finally, Worthington et al. (2011), Smith et al. (2007), and Anderson et al. (2015) merged two or more control groups, including, as we call it, an additional design.
-In an additional treatment group a standard treatment was compared to a standard treatment plus additional R/S sessions.
-This treatment group differs from the blended group, because of the difference in treatment duration, and from the alternate group due to corresponding theoretical orientation.
-Medium effect sizes (.26 < d < .59) were found these combined treatment groups, in favor of the R/S therapy (Anderson et al., 2015; Smith et al., 2007; Worthington et al., 2011).
.Moderators of Treatment Effects.
-Because of these inconsistent findings, it is important to consider potential moderators. First, as mentioned, the composition of the R/S-based treatment and the control group plays a significant role (Captari et al., 2018; Worthington et al., 2011).
-In addition to the distinction between treatment and control group, other treatment aspects can influence the results, such as the treatment setting (inpatient vs. outpatient), diagnosis treated, and religious or spiritual framework.
-Most meta-analyses use broad definitions for psychodiagnostics and psychotherapy, therefore we choose stricter inclusion criteria (a mental disorder) and opted to include diagnosis as a potential moderator.
-Secondly, several quality aspects seem to influence the ambivalent results, including methodology and researcher allegiance (Anderson et al., 2015; Paukert et al., 2011).
.Aims of the Current Meta-Analysis.
-The primary aim of the current meta-analysis was to compare R/S-based treatments to non-R/S psychotherapies.
-Strict inclusion criteria were applied to research methods, definitions of religiosity/spirituality, and the definition of psychotherapy.
-This meta-analysis focused solely on RCT’s that have been carried out in mental health care settings among participants with an official (ICD/DSM) diagnosis, to ensure a more homogeneous study population.
The secondary aim was to systematically examine several moderator variables, including study quality, to investigate whether this study can replicate and extend previous findings.
-Moreover, in contrast to most previous meta-analyses, we systematically examined the type of comparison that was made in single studies and addressed this as a potential moderator of effect size magnitude.
-The following hypotheses are tested: (i) a R/S treatment is more efficacious compared to a non-R/S treatment, in line with results from previous metaanalyses (Anderson et al., 2015; Captari et al., 2018; McCullough, 1999; Smith et al., 2007; Worthington et al., 2011); (ii) the type of comparison made and study quality moderate the difference in effect between a R/S and the control group.
-As noted, previous meta-analyses have found different results depending on the type of comparison (Anderson et al., 2015; Captari et al., 2018; McCullough, 1999; Worthington et al., 2011), therefore we expect the effect size to be moderated by the type of comparison.
-We expect that the effect size of a “blended” spiritual treatment will be lower from other types of comparisons, such as those comparing a regular therapy with the same therapy with separate R/S therapy added.
-To our knowledge, this is the first meta-analysis that addresses these types of comparisons in more detail.
-Regarding study quality, in general, this variable affects the effect sizes of randomized controlled trials (Thoma et al., 2012) and for research on R/S-based therapy in particular, quality aspects seem to influence the ambiguous outcomes (Anderson et al., 2015; Paukert et al., 2011).
-Hence, study quality is expected to moderate the results, but we have no clear predictions about this given inconsistent findings.
.Method.
^Literature Search and Identification of Studies^
-A multiple phase search was conducted in September 2014 and updated in October 2019 and January 2022 to retrieve as many RCTs as possible regarding the efficacy of religious and spiritual psychotherapy in mental health care.
-We used two search strategies to find eligible studies. First, we conducted searches in the databases Web of Science, PsycINFO, and PubMed.
-Web of Science was searched in September 2014, in October 2019, and in January 2022 using the terms: (Religio∗ OR Spirit∗ OR Existent∗ OR Christian OR Muslim OR Buddhis∗ OR Taois∗ OR Jewis∗) AND (Randomi∗ OR Psychotherapy OR Therapy OR Treatment OR Counsel∗ OR Intervention ∗ OR Outcome OR Patient∗) in the title.
-In PsycINFO and PubMed, using the same terms, only clinical trials (RCTs), reviews, and meta-analyses were searched.
-Second, the included studies in previously published meta-analyses and reviews (Anderson et al., 2015; Captari et al., 2018; Hodge, 2006; Hook et al., 2010; Lim et al., 2014; McCullough, 1999; Paukert et al., 2011; Smith et al., 2007; Viftrup et al., 2013; Vos et al., 2015; Worthington et al., 2011) were assessed.
-We contacted experts in the field of psychotherapy and religion/ spirituality by e-mail for any ongoing studies, however, this did not yield any new studies.
We did not search for unpublished manuscripts. Finally, we searched for unpublished ongoing studies in two trial registers (www.clinicaltrials.gov and www. controlled-trials.com), which yielded no results.
-As the analysis plan of the meta-analysis and the literature search took place before 2014, a pre registration of the study is missing.
.Inclusion Criteria.
-In this study, we set stringent inclusion criteria, to reduce variability among studies as much as possible.
-Included studies had to fulfill the following criteria, described according to the PICO (population, intervention, comparator, outcome) framework.
.Population.
-Patients (i) had to be 18 years or older, (ii) had to meet the official criteria for “Axis I” mental disorders according to DSM or ICD manuals, and (iii) were treated in mental health care settings.
.Intervention.
-Psychotherapeutic and counseling treatments, meeting the definition of psychotherapy according to Norcross (1990) were included, and these treatments were explicitly religious or spiritual, excluding mindfulness, meditation, yoga, due to its lack of focus on a transcendent dimension.
-In addition, only randomized controlled trials (excluding cross sectional and quasi experimental studies) were allowed.
-There were no restriction on language and publication date.
.Comparator.
-“Active” control groups were allowed for comparison, excluding wait list controls.
-In addition, due to variation in comparison treatment groups, we made the following four types of comparisons (Captari et al., 2018; Worthington et al., 2011): (i) additional comparison: a regular treatment was compared with the identical treatment except for the addition of extra religious or spiritual sessions (regular therapy compared to regular therapy + R/S therapy); (ii) blended comparison: a religious and non-religious treatments had the same theoretical orientation (e.g., CBT) and duration, but in only one group attention was paid to religious and spiritual beliefs, cognition, values and actions (for example: regular rational emotive therapy (RET) compared to R/S modified version of RET); (iii) alternative comparison: a R/S treatment was compared with an alternative treatment with a different theoretical background (for instance: CBT compared to spiritual integrated therapy); (iv) medication comparison: patients who were treated with medication were compared with patients in a R/S treatment (medication compared to R/S therapy).
.Outcome.
-Validated questionnaires and quantifiable outcome data of the main disorder under treatment were used, with at least posttreatment measurements.
-Two outcome measures were distinguished, depending on the measurements available from individual studies: (i) psychological symptoms (split into self-reported and observer-based); and (ii) functioning/well being in the broad sense (cognitive, behavioral, spiritual).
-Examples of questionnaires used: Social Adjustment Scale, Automatic Thoughts Questionnaire, Spiritual Well-Being Scale, Ways of Religious Coping Scale.
-We decided to use follow-up data at 6 months after treatment termination or nearest to 6 months, because follow-up data at 6 months were most available.
-The screening process consisted of two phases.
-Firstly, the first author screened all titles and abstracts for eligibility. After that, the first author assessed the full text articles for meeting all inclusion criteria.
-When the first author was in doubt, the studies were discussed in group meetings (GG, LE, JK, and AB) where relevant parts of the text were read and assessed until consensus was reached.
-Due to limited resources, it was not possible for the screening and data extraction to take place by two
authors.
.Data Extraction.
-The first author extracted data from each included study, specifically: basic statistics needed for effect size calculation, treatment and patient variables, therapist information, and outcome measures.
-Treatment variables were modality (group, individual or both), setting (inpatient or outpatient), treatment dosage (intensity of treatment), calculated by length of treatment in weeks multiplied by number of sessions multiplied by length of each session (in hours), and religion/spirituality (Christian, Muslim, Buddhism, spiritual, Taoist).
-Patient information consisted of diagnosis, population (e.g., patients, students, church members), percentage of women, age, and dropout (average treatment dropout of the R/S and regular treatment).
-Therapist information pertained to training (psychiatrist, psychologist/counselor, doctoral students, mental health nurse), experience, and the number of therapists in the trial.
.Quality Assessment.
-Two independent reviewers (AB and CH) assessed the quality of the studies using the Psychotherapy Quality Rating Scale (PQRS), a scale for assessing randomized clinical trials (Kocsis et al., 2010).
-This scale includes 24 items covering six quality domains and an omnibus item (question 25) to award a final score to the study. All items are scored on a threepoint scale (0–2), except item 25 (seven-point scale: 1–7).
-Two different quality scores were derived: a summative total of the individual items 1–24 (range 1–48) and an omnibus score (range 1–7).
-The judges were trained by an expert (JK).
-The one-way random intraclass correlation coefficient (ICC) (single measures) was .882 and the average measures ICC .938 (excellent).
-In the analyses, the means of the two scores were used in case of a deviation of one point, and when the deviation was two points reviewers discussed the item and reached consensus about the score.
.Data Analysis.
^Calculation of effect sizes^
-The analyses were performed using R-Studio software version 2023.03.0 (Build386). Two functions of R were used: the rma.mv function of the metafor package (Viechtbauer, 2015) to fit multi-level meta-analytic models and the metagen function of the meta package (Balduzzi et al., 2019) for plots.
-Because of dependence of effect sizes of included studies, resulting in unit-of-analysis problems and double-counting problems, we used a multi-level meta-analytic model (Harrer et al., 2021).
-A multi-level model allows all the relevant effect sizes reported in the individual studies to be included. -Assink and Wibbelink (2016) describe in a step-by-step tutorial how to perform a three-level meta analytic model with the rma.mv function in R. In addition, using the metagen package, separate effect sizes were calculated for symptoms and functioning posttreatment and follow-up, and prediction intervals were assessed.
-A prediction interval quantifies the uncertainty associated with making individual predictions and indicates what effects are to be expected for future patients (IntHout et al., 2016).
-It provides an estimated range within which the true value of an individual observation is likely to fall, taking into account both the inherent variability in the data and the uncertainty in the prediction model.
-We also generated forest plots and funnel plots with this package.
-Between group effect sizes (Hedges’ g) were calculated by comparing means, standard deviations and sample sizes of the R/S-based treatments with the regular treatments at post-treatment and follow-up.
-In studies that compared two or more therapies, the sample size of the shared group was split, to avoid the problem of double counting (Harrer et al., 2021).
-To calculate the pooled effect sizes per domain, the n was divided by the number of questionnaires used in the study.
-Effect sizes of < .30 are considered small, .50 medium, and >.80 large (Cohen, 1977).
-A random effects model was used to compute weighted mean effect sizes, because samples, treatment interventions, population, and methodologies were expected to vary across studies.
-The random effects model results in more conservative results and broader 95%-confidence intervals (95% CI) than the fixed effects model.
-To estimate the parameters in the multi-level model, the Restricted Maximum Likelihood method (REML) was used (Viechtbauer, 2005), and a Knapp-Hartung adjustment (Knapp & Hartung, 2003) of the confidence interval was applied. The following effect sizes were calculated: overall (symptoms + functioning) effect sizes posttreatment (in rma.mv), psychological symptoms posttreatment and follow-up (in metagen), and posttreatment effect sizes for the functioning outcomes (in metagen).
.Heterogeneity.
-In order to test for heterogeneity, one-sided log-likelihood-ratio-tests were performed in rma.mv to test variance (Assink & Wibbelink, 2016).
-Three sources of variance are distinguished in the multi-level model:
-Level 1: sample variance of the effect sizes;
-Level 2: variance between effects sizes within one study (e.g., due to subgroups within a study or different outcome domains);
-Level 3: variance between studies. Significant results on the second and third level indicate heterogeneous distribution of the effect sizes.
-In that case, differences in effect sizes could be explained by study characteristics, which can be further investigated by moderator analyses.
.Moderator analysis.
-Instructions from Assink and Wibbelink (2016) regarding moderator analysis were used.
-Dummy variables were created for the categorical variables (assessment perspective, domains, type of comparison, religion, diagnosis, population, modality, and setting) and the dimensional variables (study quality, mean age, percentage gender, percentage dropout, treatment doses) were centered around the mean.
-The results of the moderator analyses include: (i) an omnibus test of moderators, based on the F distribution, to assess whether a variable moderates the difference in effect size between a R/S and non R/S treatment, i.e. to test significant differences between the levels of a moderator, and (ii) a model result showing whether a level (reference category) within a moderator individually deviate from zero, and whether the other levels differ from the reference category, based on the t distribution.
.Publication bias.
-Publication bias denotes the problem that non-significant studies could be unpublished, potentially resulting in biased meta-analytic findings.
-Several methods were used to test for publication bias.
-Funnel plots were visually inspected, and Egger’s regression and the Duval and Tweedie’s trim and fill procedure were calculated.
-Publication bias was tested with the metagen package for psychological symptoms and functioning posttreatment.
.Results.
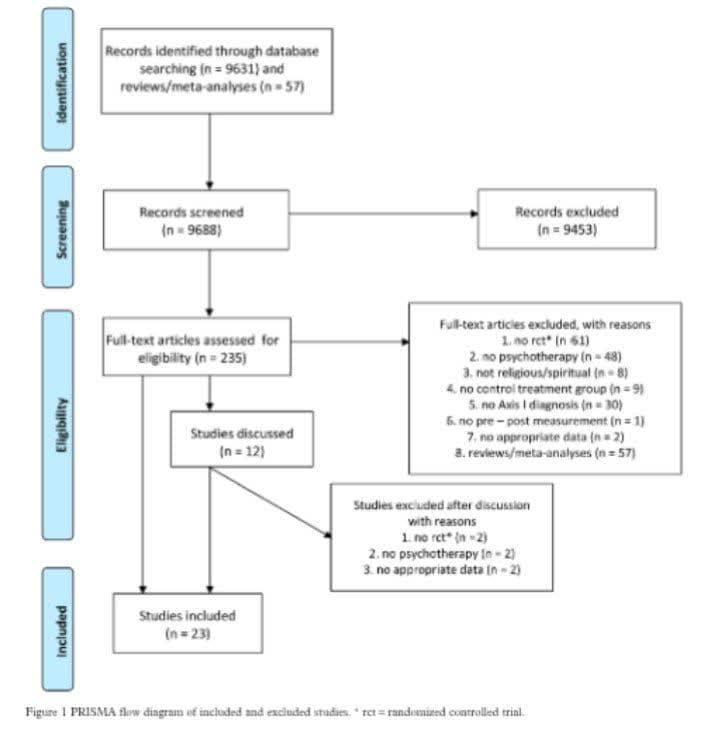
^Study Selection^
-Figure 1 shows the flow chart of the selection procedure: 9688 articles were screened and, of these, 9453 were discarded based on title and 248 based on abstract. A total of 235 full-text articles were assessed for eligibility, of which 206 were excluded, 17 were included and 12 studies were discussed in group meetings.
-A description of the discussion and decision-making process can be found in Supplement4.
.Descriptive Characteristics of Studies.
^Treatments of the included studies.^
-Twentythree studies were included in the meta-analysis with a total of 1499 clients (R/S treatment: n = 768; non-R/S treatment: n = 731). In total, 27 comparisons could be made from which k = 83 posttreatment effect sizes were extracted and k = 28 follow-up effect sizes.
-Razali et al. (1998) and Zhang et al. (2002) evaluated two studies in their articles and in the studies of Ebrahimi et al. (2013) and Richards et al. (2006) a spiritual group was compared with 2 alternative treatments.
-Six treatments had a Muslim tradition (n = 245), eight Christian (n = 159), one Taoist (n = 95), one Buddhist (n = 58) and seven general spiritual tradition (n = 223).
-Detailed information about the treatment offered can be found in Supplement 1.
-In summary, 16 studies pertained to outpatient treatments, four studies examined inpatients, and three studies lacked information about the setting. Of these 16 studies involving outpatients, five treatments were offered in group therapy (average of 8.2 sessions), eight studies pertained to individual sessions (average of 10.88 sessions), two studies combined individual and group sessions and one study lacked information.
-The amount of studies in each type of comparison was: (i) additional: 15 studies (n = 581); (ii) blended: 6 studies (n = 85); (iii) alternative: 3 comparisons (n = 39); and (iv) medication: 3 studies (n = 97). Patients in the blended and alternative comparison group received equal dosage of therapy sessions.
.Patient characteristics in the included studies.
-A variety of disorders were treated in the studies: depression (s = 10); dysthymic disorder (s = 3); generalized anxiety disorder (s = 7); eating disorders (s = 3); substance abuse (s = 2), and 2 studies treated multiple disorders. The average age of participants was 34.5 years (5 studies lacked data) and 57%were women (7 studies missing data).
-Patients were involved in 74.1% of the comparison groups, the remainder of participants were drawn from student samples and the general population (25.9%).
.Therapist characteristics in the included studies.
-In four studies the therapist was a psychiatrist, in four a doctoral student provided the treatment, in two studies a psychologist was involved, in three studies a mental health nurse and in two a counselor was involved.
-In only five articles the therapists were described as experienced, and four studies reported that the therapists were trained and supervised in the provided treatment.
-In five studies, the therapist treats both treatment groups. The number of therapists involved was usually one or two, however, three studies involved more than three therapists.
-Two studies provided an evaluation of the treatment and evaluation of the therapeutic relationship was absent in all studies.
-Seven studies did not contain any information about the therapists involved.
-A minority of studies (17%) paid attention to allegiance of therapists to the type of treatment.
-In these cases, the therapists treated both treatment groups and were not involved in the development of the R/S treatment.
-However, in all these studies the authors or supervisors developed the R/S therapy.
.Methodological quality of the included studies.
-The mean methodological quality across the 23 studies according to the PQRS was 19.
-This indicates an overall “rather poor” study quality and falls below the score of 24 reflecting “adequate quality.” Six of the included studies had a score above 23.
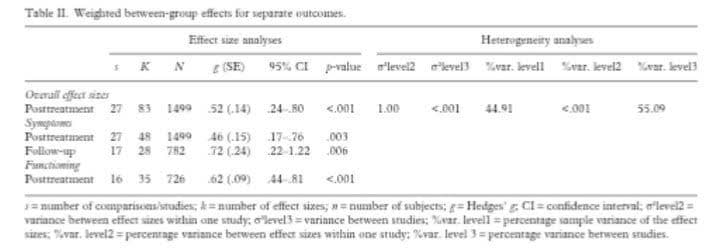
.Effect Sizes Overall R/S versus regular treatment.
-The first aim of this meta-analysis was to compare the efficacy of a R/S treatment to religious/spiritual patients with the efficacy of a regular treatment post-treatment (Table II).
-The overall effect size was Hedges’ g = .52 (SE = .14, t(82) = 3.68, p < .001), 95% CI = 0.24–0.80, PI (−0.76–1.81) at posttreatment, indicating that a R/S treatment is moderately more efficacious compared to a regular therapy.
-Results of the log-likelihood-ratio-tests, assessing heterogeneity, revealed significant variability between studies (level 3), 55.09% of the total variance could be attributed to differences between studies (p < .001).
Within-study variance was mainly found at level 1 (sampling variance) (44.91%).
.Psychological symptoms R/S versus regular treatment.
-Significant effects on psychological symptoms were found at posttreatment (g = .44,SE = .13, t(48) =3.36, p < .01, 95% CI = 0.17–0.70), of which 7 outliers were detected in six studies (Barron, 2007; Chida et al.,2016; Razali et al., 2002; Shanke et al., 2017; Tonkin, 2005;Zhang et al., 2002).
-After removing these outliers, the significant result remained (g = .43, t(41) =6.20, p < .001, 95% CI = 0.29–0.57).
-Figure 2 shows the funnel plot of the symptom results, and the appendix contains the forest plot (Supplement2) including the prediction interval (PI = −1.14–2.01).
-The superiority of a R/S treatment was maintained over longer time frames, considering the follow-up results (g = .72, SE = .24, t(27) = 2.98, p< .01, 95% CI = 0.22–1.22).
.Functioning R/S versus regular treatment.
-Posttreatment effect sizes for functioning, with one outlier (Miller et al., 2008), also demonstrated the efficacy of a R/S-based therapy over a non-R/S treatment (g = .62, SE = .09, t(35) = 6.82, p < .01, 95% CI = 0.44–0.81) (see Figure 3 the funnel plot and in the appendix the forest plot (S3)), including the prediction intervals, which does not contain zero (PI = 0.03–1.21). Follow-up results were not available for this outcome domain.
.Moderators.
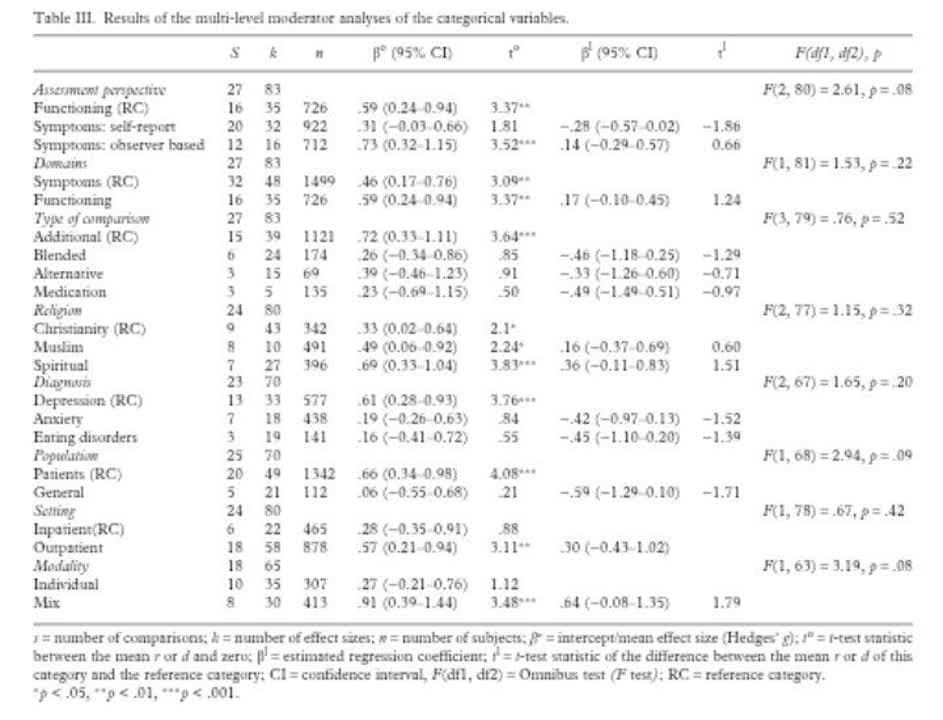
-Tables III and IV show the results of the univariate moderator analyses comparing R/S treatment with regular treatment.
-The results of the omnibus tests of moderators showed no significant differences for any of the potential moderator variables (p values of the F distributions > .05), meaning that the overall effect size is not moderated by any of the categorical and continuous moderator variables.
-The model results of the moderator analyses did show differences within variables, that is, for some levels within a variable significant effect sizes (βo and to) were found between a R/S-based therapy and
regular therapy.
-For example, for assessment perspective, the level observer-based symptoms and functioning were both significantly different from zero, but this was not the case for self-reported symptoms.
-This implies that the reported differences between the R/S and non-R/S treatment groups applies only to observer-based symptoms and functioning.
-Both domains,symptoms, and functioning, deviated significantly from zero, meaning that there was no distinction between symptoms and functioning concerning the superiority of R/S-based therapy.
-Only the additional type of comparison group showed a significant deviation, indicating that the reported differences only apply to the additional comparison group.
-Moreover, for the moderator diagnosis, effect sizes of anxiety and eating disorders were not significant while studies that treated depressed patients the R/S treatment differed significantly from a non-R/S therapy.
-This implies that our results only apply to depressed patients.
-All religions deviated significantly from zero, meaning that our results concerning the superiority of R/Sbased therapy apply to all religions tested. Finally, R/S-based therapy outperformed regular therapy in
case of patients (compared to general population), outpatients (compared to inpatients), and treatments
combining individual and group therapy (compared to individual therapy).

.Publication Bias.
-Publication bias was tested for psychological symptoms and functioning at posttreatment.
-First, visual inspection of the funnel plots did not indicate potential bias, although asymmetry is visible on the right side of the two plots.
-Secondly, Egger’s Regression Test (Egger et al., 1997) showed that the intercept of the variable symptoms (βo = −.39,p = .59) and functioning (βo = −.83, p = .13) did not deviate significantly from zero, implying that the funnel plots are indeed symmetric.
-Duval and Tweedie’s trim and fill method showed that symmetry in the funnels plots was restored by imputing 17 symptom effect sizes from 11 studies, and 9 effect sizes (6 studies) for functioning.
-All effect sizes were imputed on the right side of the plots, meaning an overrepresentation of below average findings.
-In sum, there appears to be some publication bias, however, from studies with below average results.
.Discussion.
-The first purpose of this meta-analysis was to compare a R/S-based therapy to non-R/S treatments.
-The hypothesis that religious or spiritual patients benefit more from a R/S therapy compared to non-R/S therapy was confirmed in this meta-analysis.
-Moderate effect sizes were found overall (g = .52) and for symptom reduction (g = .44), comparable to previous meta-analytic findings that reported effects between d = .13 – d = .59 for reducing complaints
(Anderson et al., 2015; Captari et al., 2018; McCullough, 1999; Smith et al., 2007; Worthington et al., 2011). -R/S treatments not only reduce complaints more, but also enhance general functioning(g = .62) (to compare: d = .41 in Worthington et al.
-[2011] and g = .43 in Captari et al. [2018]).
-Interestingly, as indicated by the prediction intervals in both domains, the estimate of functioning (PI = .03–1.21) was more robust than that of symptoms (PI = -.76–1.81). In the case of functioning, the interval does not contain zero, which implies that R/S interventions will most likely be efficacious in this domain
for future patients.
-This fits with the more personalized approach which is inherent in R/S treatment, where the focus does not lie primarily on symptoms.
-In other words, this meta-analysis affirms the beneficial effects of person-centered treatments in which religious and spiritual experiences, language, and worldviews of patients are recognized and explicitly
addressed.
-We suspect that an explanation can be found in the person-centered approach that focuses on the person as a whole and sees the experience and alleviation of psychological distress as a personal
journey, or narrative, with an inherent existential dimension (Glas, 2021).
-Our meta-analysis corroborates the view that openness and willingness to address the spiritual, religious, and existential aspects of the patient’s suffering are associated with feelings of being recognized accepted, and understood as a person.
-Although the underlying mechanisms are not well understood, this open and encouraging attitude invites using a spiritually more inclusive vocabulary which might positively affect the therapeutic relationship (van Os et al., 2019).
-It also emphasizes the importance to foster awareness in clinicians of their R/S identity in training and supervision, as this is an area where psychotherapists feel they lack competence (Magaldi & Trub, 2018). –In fact, dealing with self-disclosure of (parts of) their own R/S identity may enhance openness and thus strengthen the therapeutic relationship.
-Yet, our study does not answer the question how the various and complex ways in which worldviews of both patient and clinician interact and how this interaction may influence treatment results.
-This topic deserves further study.
.Implication of the Moderator Findings.
-The moderator analyses yielded interesting exploratory results, but these results should be evaluated
taking into account the (limited) statistical power per moderator.
-First, that the type of comparison would be a significant moderator of effect, as suggested by previous meta-analyses, could not be replicated in the current meta-analysis.
-The omnibus moderator test yielded no significant result.
-However, of all type of comparisons, only the effect size of the additional group differed significantly.
-As was shown in this and three previously published meta-analyses, a “blended” treatment does not appear to show a significant effect compared to its non-blended counterparts (Captari et al., 2018; McCullough, 1999; Worthington et al., 2011; see however Anderson et al., 2015).
-However, there seems to be more differentiation in the types of comparisons that were merged by earlier meta-analyses (Table I), including the distinction between an additional and alternative design.
-This may explain some of the inconsistent results from previous meta-analyses.
-Importantly, however, it should be noted that statistical power is a major problem in this comparison, as the alternative groups consists of only 69 patients.
-Further research is needed to gain more clarity on whether the method of integrating religion and spirituality into treatments affects the efficacy of psychotherapy.
-Secondly, the overall effect size comparing a R/S-based therapy to a general therapy seems especially applicable to treatments of depressed patients.
-This exploratory analysis suggests that depressive patients in particular benefit from treatments in which religious and spiritual subjects are part of a mental health treatment.
-Aspects of R/S are closely intertwined with risk of depressive symptoms, coping with, and the course and recovery from depression (Braam & Koenig, 2019).
-Positive aspects of R/S, including prayer, church attendance and social support, as well as discussing spiritual struggles, reflecting on life values and existential meaning, can promote recovery from depression (Hittner & Swickert, 2010).
-Secondly, the overall effect size of selfreported symptoms is not significant, while observer-
based symptoms and functioning are.
-Several explanations are given for the discrepancy between observer and self-reported symptoms, for example,personality factors, personality characteristics, and psychiatric history (Schat et al., 2017).
-Finally, we hypothesized that study quality would moderate the difference in effect between R/S and non-R/S treatment.
-This was not confirmed in this meta-analysis; an overall study quality measure did not explain the
difference in efficacy.
-In conclusion, the results of the moderator analyses point toward some directions for further research.
.Limitations.
-The results of this meta-analysis have to be interpreted within the context of several theoretical and procedural limitations.
-First, the mean methodological quality of the included studies was “rather poor.” This may influence the results (Thoma et al., 2012), although no association was found between the overall study quality and treatment results.
-Highquality randomized controlled trials are needed to increase the reliability of the efficacy of R/S-based treatments. Second, the moderators are not always unambiguous and therefore reliable.
-For example, studies lack information about the moderators, allegiance bias is present, the absence of various religions (Jewish, Buddhism), the approach of integrating religion in psychotherapy, and some moderators appear to overlap, such as type of comparison and religion.
-In addition, potential mediating variables that explain the effectiveness of psychotherapy in general, and a R/S treatment in particular, are missing, such as client factors (motivation and involvement in therapy), patients’ preference, and quality of the therapeutic relationship (Cooper, 2008).
-We recommend researchers to include these variables in further research to explain the efficacy of R/S treatments.
-Thirdly, although this meta-analysis tried to create a homogeneous research group, the studies differ on various variables, which raises the question whether comparing these studies with each other does full justice to their individual aspects.
-The studies differ, for example, in the severity of the complaints, psychotherapy orientations, content of the R/S treatment, control group and location.
-Not all of these factors could be included as moderators.
-Further, the meta-analysis did not include a measure of the importance of spirituality to patients and their religious motivation, while studies show, for example, that the onset and course of psychopathology differ in patients who are intrinsically or extrinsically religious motivated (Park, 2021).
-It is likely that patients sought help at institutions with religious affiliation with good reason, and this may have introduced an important bias.
-Specifically, it may have resulted in underestimated effects for the control groups due to patients’ unfulfilled needs to talk about religion.
-This topic requires further attention as religious motivation may affect the outcome of a R/S treatment.
-Fifth, this meta-analysis is based on a traditional mental health care system, with categorical diagnosis, an official DSM diagnosis and evidence-based treatments.
However, the approach within mental health care is increasingly broader, with more emphasis on dimensionalizing of mental illnesses and transdiagnostic factors (Krueger & Eaton, 2015).
-This broader approach may yield a more comprehensive picture, also with respect to severity of illness.
-Regarding the procedural limitations, all studies were searched and included by one author, which
may have compromised the reliability of the search.
-Second, in the absence of data on the studies, the authors were not contacted to complete this information or were not given access to all potential eligible research reports. Further, to assess study quality, we took the sum scale score, and this overall rating may miss key elements, such as allegiance (Jüni et al., 1999).
-Finally, pre-registration of the meta-analysis was lacked.
-Despite some limitations mentioned, this metaanalysis yields new insights, compared to previous meta-analyses, by providing a more homogeneous base of primary studies, (with strict criteria regarding a DSM diagnosis, psychotherapy, and spiritual topics of a R/S-based treatment).
-Second, we evaluated treatment effects in several domains.
-Third, we included a number of moderators, for example by looking in some detail into varieties of control groups.
.Conclusions.
-This meta-analysis supports the hypothesis that a R/S-based treatment is more efficacious than regular
treatment in mental health care settings for patients with religious affiliations.
-This type of person-centered treatment focused on the religious, spiritual and existential dimensions of human beings is efficacious in reducing psychological symptoms and enhancing general functioning, in particular for depressed patients. We, therefore, advocate that clinicians and mental health care providers should discuss patients’ worldviews, expressed in religious and spiritual subjects, in psychotherapy.
-More research is needed into the role of the type of comparison and the way in which religious and spiritual topics should be integrated in psychotherapy.
-We encourage future research on R/S psychotherapy to adhere to developments toward person-centered and holistic therapeutic approaches.
-Finally, we recommend that future studies focus on mechanisms of change in R/S psychotherapeutic treatment, as this is an essential step toward improving psychotherapy further.
.Funding.
-This research did not receive any specific grant from funding agencies in the public, commercial, or notfor-profit sectors.
.Disclosure Statement.
-No potential conflict of interest was reported by the author(s).
.Supplemental data.
-Supplemental data for this article can be accessed online at https://doi.org/10.1080/10503307.2023.
2241626.
.Contributors.
-A.J. Bouwhuis-van Keulen: conceptualization, writing – original draft, literature search, data curation, quality assessment, methodology, formal analysis, visualization. J. Koelen: conceptualization,
writing – review and editing, supervision, methodology, formal analysis.
-E.H.M. Eurelings: conceptualization, writing – review, and editing. C.Hoekstra-Oomen: quality assessment, writing –review and editing. G. Glas: conceptualization,writing – review, and editing.
.References.
-References marked ∗ are studies included in the meta-analysis.
-American Psychological Association. (2017). Multicultural guidelines:
An ecological approach to context, identity, and intersectionality.
Retrieved March 4, 2021, from http://www.apa.org/about/ policy/multicultural-guideline.pdf.
-Anderson, N., Heywood-Everett, S., Siddiqi, N., Wright, J.,
Meredith, J., & McMillan, D. (2015). Faith-adapted psychological
therapies for depression and anxiety: Systematic
review and meta-analysis. Journal of Affective Disorders, 176,
183–196. https://doi.org/10.1016/j.jad.2015.01.019
-Ano, G. G., & Vasconcelles, E. B. (2005). Religious coping and
psychological adjustment to stress: A meta-analysis. Journal of
Clinical Psychology, 61(4), 461–480. https://doi.org/10.1002/ jclp.20049
-Assink, M., & Wibbelink, C. J. M. (2016). Fitting three-level
meta-analytic models in R: A step-by-step tutorial. The
Quantitative Methods for Psychology, 12(3), 154–174. https:// doi.org/10.20982/tqmp.12.3.p154
-∗Azhar, M. Z., & Varma, S. L. (1995a). Religious psychotherapy
as management of bereavement. Acta Psychiatrica
Scandinavica, 91(4), 233–235. https://doi.org/10.1111/j.1600- 0447.1995.tb09774.x
-∗Azhar, M. Z., & Varma, S. L. (1995b). Religious psychotherapy
in depressive patients. Psychotherapy Psychosomatics, 63(3–4),
165–168. https://doi.org/10.1159/000288954
-∗Azhar, M. Z., Varma, S. L., & Dharap, A. S. (1994). Religious
psychotherapy in anxiety disorder patients. Acta Psychiatrica
Scandinavica, 90(1), 1–3. https://doi.org/10.1111/j.1600- 0447.1994.tb01545.x
-Balduzzi, S., Rücker, G., & Schwarzer, G. (2019). How to
perform a meta-analysis with R: A practical tutorial. Evidence
Based Mental Health, 22(4), 153–160. https://doi.org/10.1136/ ebmental-2019-300117
-∗Barron, L. W. (2007). Effect of religious coping skills training with
group cognitive behavioral therapy for treatment of depression
[Unpublished doctoral dissertation], Northcentral University,
Prescott, Arizona.
-Braam, A. W., & Koenig, H. G. (2019). Religion, spirituality and
depression in prospective studies: A systematic review. Journal
of Affective Disorders, 257, 428–438. https://doi.org/10.1016/j. jad.2019.06.063
-Captari, L. E., Hook, J. N., Hoyt, W., Davis, D. E.,
McElroy-Heltzel, S. E., & WorthingtonJr.E. L. (2018).
Integrating clients’ religion and spirituality within psychotherapy:
A comprehensive meta-analysis. Journal of Clinical Psychology, 74
(11), 1938–1951. https://doi.org/10.1002/jclp.22681
-∗Chida, Y., Schrempft, S., & Steptoe, A. (2016). A novel religious/
spiritual group psychotherapy reduces depressive symptoms in
a randomized clinical trial. Journal of Religion and Health, 55(5),
1495–1506.https://doi.org/10.1007/s10943-015-0113-7
-Cohen, J. (1977). Statistical power analysis for the behavioural
sciences. Academic Press.
-Cooper, M. (2008). Essential research findings in counselling and psychotherapy:
The facts are friendly. British Association for Counselling and Psychotherapy.
-∗Ebrahimi, A., Neshatdoost, H. T., Mousavi, S. G., Asadollahi,
G. A., & Nasiri, H. (2013). Controlled randomized clinical
trial of spirituality integrated psychotherapy, cognitive-behavioral
therapy and medication intervention on depressive symptoms
and dysfunctional attitudes in patients with dysthymic
disorder. Advances Biomedical Research, 2(1), 1–7. https://doi. org/10.4103/2277-9175.114201
-Egger, M., Davey-Smith, G., Schneider, M., & Minder,
C. (1997). Bias in meta-analysis detected by a simple, graphical
test. British Medical Journal, 315, 629–634. https://doi.org/10. 1136/bmj.315.7109.629
-Glas, G. (2019). Person-centered care in psychiatry. Self-relational,
contextual, and normative perspectives. Routledge.
Glas, G. (2021). Models of integration of christian worldview and
psychiatry. In J. R. Peteet, H. S. Moffic, A. Hankir, & H. G.
Koenig (Eds.), Christianity and psychiatry (pp. 163–180).
Springer International Publishing.
-Harrer, M., Cuijpers, P., Furukawa, T. A., & Ebert, D. D. (2021).
Doing meta-analysis with R. A hands-on guide. Chapmann &
Hall/CRC Press. Welcome! | Doing Meta-Analysis in R
(bookdown.org).
-Hittner, J. B., & Swickert, R. (2010). Discriminant ability of the
sense of coherence scale: Manageability, meaningfulness, and
comprehensibility as classifiers of depression. Individual
Differences Research, 8(3), 171–175.
-Hodge, D. R. (2006). Spiritually modified cognitive therapy: A
review of the literature. Social Work, 51(2), 157–166. https:// doi.org/10.1093/sw/51.2.157
-Hook, J. N., WorthingtonJr.E. L., Davis, D. E., JenningsII, D. J.,
Gartner, A. L., & Hook, J. P. (2010). Empirically supported
religious and spiritual therapies. Journal of Clinical Psychology,
66(1), 46–72. https://doi.org/10.1002/jclp.20626
-∗Hsiao, F. H., Jow, G. M., Lai, Y. M., Chen, Y. T., Wang, K. C.,
Ng, S. M., Ho, R. T. H., Chan, C. L. W., & Yang, T. T.
(2011). The long-term effects of psychotherapy added to pharmacotherapy
on morning to evening diurnal cortisol patterns in
outpatients with major depression. Psychotherapy and
Psychosomatics, 80(3), 166–172. https://doi.org/10.1159/ 000321558
-IntHout, J., Ioannidis, J. P. A., Rovers, M. M., & Goeman, J. J.
(2016). Plea for routinely presenting prediction intervals in
meta-analysis. BMJ Open, 6(7), e010247. https://doi.org/10. 1136/bmjopen-2015-010247
-∗Johnson, W. B., DeVries, R., Ridley, C. R., Pettorini, D., &
Peterson, D. R. (1994). The comparative efficacy of
Christian and secular rational-emotive therapy with Christian
clients. Journal of Psychology and Theology, 22(2), 130–140.
https://doi.org/10.1177/009164719402200206
-∗Johnson, W. B., & Ridley, C. R. (1992). Brief Christian and
non-Christian rational-emotive therapy with depressed
Christian clients: An exploratory study. Counseling and
Values, 36(3), 220–229. https://doi.org/10.1002/j.2161- 007X.1992.tb00790.x
-Jüni, P., Witschi, A., Bloch, R., & Egger, M. (1999). The hazards
of scoring the quality of clinical trials for meta-analysis. The
Journal of the American Medical Association, 282(11), 1054
-Knapp, G., & Hartung, J. (2003). Improved tests for a random
effects meta-regression with a single covariate. Statistics in
Medicine, 22(17), 2693–2710. https://doi.org/10.1002/sim. 1482
-Kocsis, J. H., Gerber, A. J., Milrod, B., Roose, S. P., Barber, J.,
Thase, M. E., Perkins, P., & Leon, A. C. (2010). A new
scale for assessing the quality of randomized controlled
clinical trials of psychotherapy. Comprehensive Psychiatry,
51(3), 319–324. https://doi.org/10.1016/j.comppsych.2009. 07.001
-∗Koszycki, D., Bilodeau, C., Raab-Mayo, K., & Bradwejn, J.
(2014). A multifaith spiritually based intervention versus supportive
therapy for generalized anxiety disorder: A pilot randomized
controlled trial. Journal of Clinical Psychology, 70(6),
489–509. https://doi.org/10.1002/jclp.22052
-∗Koszycki, D., Raab, K., Aldosary, F., & Bradwejn, J. (2010). A
multifaith spiritually based intervention for generalized
anxiety disorder: A pilot randomized trial. Journal of Clinical
Psychology, 66(4), 430–441. https://doi.org/10.1002/jclp. 20663
-Krueger, R. F., & Eaton, N. R. (2015). Transdiagnostic factors of
mental disorders. World Psychiatry, 14(1), 27–29. https://doi. org/10.1002/wps.20175
-Lim, C., Sim, K., Renjan, V., Sam, H. F., & Quah, S. L. (2014).
Adapted cognitive-behavioral therapy for religious individuals
with mental disorder: A systematic review. Asian Journal of
Psychiatry, 9, 3–12. https://doi.org/10.1016/j.ajp.2013.12.011
-Magaldi, D., & Trub, L. (2018). (What) do you believe?:
Therapist spiritual/religious/non-religious self-disclosure.
Psychotherapy Research, 28(3), 484–498. https://doi.org/10. 1080/10503307.2016.1233365
-∗Margolin, A., Beitel, M., Schuman-Olivier, Z., & Avants, S. K.
(2006). A controlled study of a spirituality-focussed intervention
for increasing motivation for HIV prevention among
drug users. AIDS Education and Prevention, 18(4), 311–322.
https://doi.org/10.1521/aeap.2006.18.4.311
-McCullough, M. E. (1999). Research on religion-accommodative
counseling: Review and meta-analysis. Journal of Counseling
Psychology, 46(1), 92–98. https://doi.org/10.1037/0022-0167. 46.1.92
-∗Miller, W. R., Forcehimes, A., O’Leary, M. J., & LaNoue, M. D.
(2008). Spiritual direction in addiction treatment: Two clinical
trials. Journal of Substance Abuse Treatment, 35(4), 434–442.
https://doi.org/10.1016/j.jsat.2008.02.004
-Norcross, J. C. (1990). An eclectic definition of psychotherapy. In
J. K. Zeig, & W. M. Munion (Eds.), What is psychotherapy?
Contemporary perspectives (pp. 218–220). Jossey-Bass.
Pargament, K. I. (2007). Spiritually integrated psychotherapy.
Understanding and addressing the sacred. The Guilford Press.
Park, C. L. (2021). Intrinsic and extrinsic religious motivation:
Retrospect and prospect. The International Journal for the
Psychology of Religion, 31(3), 213–222. https://doi.org/10. 1080/10508619.2021.1916241
-Paukert, A. L., Phillips, L. L., Cully, J. A., Romero, C., & Stanley,
M. A. (2011). Systematic review of the effects of religiousaccommodative
psychotherapy for depression and anxiety.
Journal of Contemporary Psychotherapy, 41(2), 99–108. https:// doi.org/10.1007/s10879-010-9154-0
-∗Pecheur, D. R., & Edwards, K. J. (1984). A comparison of
secular and religious versions of cognitive therapy with
depressed Christian college students. Journal of Psychology
and Theology, 12(1), 45–54. https://doi.org/10.1177/ 009164718401200106
-Pew Research Centre. (2015, April 2). The future of world religions:
Population growth projections, 2010-2050. Department Religion.
https://www.pewresearch.org/religion/2015/04/02/religiousprojections- 2010-2050/#fn-22652-1.
-∗Propst, L. R., Ostrom, R., Watkins, P., Dean, T., & Mashburn,
D. (1992). Comparative efficacy of religious and nonreligious
cognitive-behavioral therapy for the treatment of clinical
depression in religious individuals. Journal of Consulting and
Clinical Psychology, 60(1), 94–103. https://doi.org/10.1037/ 0022-006X.60.1.94
-∗Razali, S. M., Aminah, K., & Khan, U. A. (2002). Religious-cultural
psychotherapy in the management of anxiety patients.
Transcultural Psychiatry, 39(2), 130–136. https://doi.org/10. 1177/136346150203900106
-∗Razali, S. M., Hasanah, C. I., Aminah, K., & Subramaniam, M.
(1998). Religious-sociocultural psychotherapy in patients with
anxiety and depression. Australian and New Zealand Journal of
Psychiatry, 32(6), 867–872. https://doi.org/10.3109/ 00048679809073877
-∗Rentala, S., Fong, T. C. T., Nattala, P., Chan, C. L. W., &
Konduru, R. (2015). Effectiveness of body-mind-spirit intervention
on well-being, functional impairment and quality of
life among depressive patients – A randomized controlled
trial. Journal of Advanced Nursing, 71(9), 2153–2163. https:// doi.org/10.1111/jan.12677
-Richards, P. S., & Bergin, A. E. (2005). A spiritual strategy for counseling
and psychotherapy (2nd ed). American Psychological
Association.
-∗Richards, P. S., Berrett, M. E., Hardman, R. K., & Eggett, D. L.
(2006). Comparative efficacy of spirituality, cognitive, and
emotional support groups for treating eating disorder inpatients. Eating Disorders, 14(5), 401–415. https://doi.org/10.1080/10640260600952548
-Schaap-Jonker, H., van der Velde, N., Eurelings-Bontekoe,
E. H. M., & Corveleyn, J. M. T. (2017). Types of god representation
and mental health: A person-oriented approach. The
International Journal for the Psychology of Religion, 27(4), 199–
-Schat, A., van Noorden, M. S., Giltay, E. J., Noom, M. J.,
Vermeiren, R. R. J. M., & Zitman, F. G. (2017).
Concordance between self-reported and observer-rated
anxiety severity in outpatients with anxiety disorders: The
Leiden routine outcome monitoring study. Psychology and
Psychotherapy: Theory, Research and Practice, 90(4), 705–719.
https://doi.org/10.1111/papt.12134
-∗Shanke, A., Kalal, K., Save, D., & Sarve, P. (2017). Evaluation of
the effect of spiritual care on patients with generalized anxiety
and depression: A randomized controlled study. Psychology,
Health & Medicine, 22(10), 1186–1191. https://doi.org/10. 1080/13548506.2017.1290260
-Smith, T. B., Bartz, J., & Richards, P. S. (2007). Outcome of religious
and spiritual adaptation to psychotherapy: A meta-analytic
review. Psychotherapy Research, 17(6), 643–655. https:// doi.org/10.1080/10503300701250347
-∗Sreevani, R., Reddemma, K., Chan, C. L. W., Leung, P. P. Y.,
Wong, V., & Chan, C. H. Y. (2013). Effectiveness of integrated
body-mind-spirit group intervention on the well-being of
Indian patients with depression: A pilot study. The Journal of
Nursing Research, 21(3), 178–185. https://doi.org/10.1097/jnr. 0b013e3182a0b041
-Stulp, H. P., Koelen, J., Schep-Akkerman, A., Glas, G. G., &
Eurelings-Bontekoe, E. H. M. (2019). God representations
and aspects of psychological functioning: A meta-analysis.
Cogent Psychology, 6(1), 1647926. https://doi.org/10.1080/ 23311908.2019.1647926
-Thoma, N. C., McKay, D., Gerber, A. J., Milrod, B. L., Edwards,
A. R., & Kocsis, J. H. (2012). A quality-based review of randomized
controlled trails of cognitive-behavioral therapy for
depression: An assessment and metaregression. The American Journal of Psychiatry, 169(1), 22–30. https://doi.org/10.1176/appi.ajp.2011.11030433
-∗Tonkin, K. M. (2005). Obesity, bulimia, and binge-eating disorder:
The use of a cognitive behavioral and spiritual intervention
[Unpublished doctoral dissertation], Bowling Green State
University, OH.
-van Os, J., Guloksuz, S., Vijn, T. W., Hafkenscheid, A., &
Delespaul, P. (2019). The evidence-based group-level
symptom-reduction model as the organizing principle for
mental health care: Time for change? World Psychiatry, 18(1),
88–96. https://doi.org/10.1002/wps.20609
-Viechtbauer, W. (2005). Bias and efficiency of meta-analytic variance
estimators in the random-effects model. Journal of
Educational and Behavioral Statistics, 30(3), 261–293. https:// doi.org/10.3102/10769986030003261
-Viechtbauer, W. (2015). Conducting meta-analyse in R with
the metafor package. Journal of Statistical Software, 36(3),
1–48.
-Viftrup, D. T., Hvidt, N. C., & Buus, N. (2013). Spiritually and
religiously integrated group psychotherapy: A systematic literature
review. Evidence-Based Complementary and Alternative
Medicine, 2013-10-31(article ID 274625-12), https://doi.org/ 10.1155/2013/274625
-Vos, J., Craig, M., & Cooper, M. (2015). Existential therapies: A
meta-analysis of their effects on psychological outcomes.
Journal of Consulting and Clinical Psychology, 83(1), 115–128.
https://doi.org/10.1037/a0037167
-Worthington, E. L., Hook, J. N., Davis, D. E., & McDaniel,
M. A. (2011). Religion and spirituality. In J. C. Norcross
(Ed.), Psychotherapy relationships that work: Evidence based
responsiveness (2nd ed.) (pp. 402–421). Oxford University
Press.
-∗Zhang, Y., Young, D., Lee, S., Li, L., Zhang, H., Xiao, Z., Hao,
W., Feng, Y., Zhou, H., & Chang, D. F. (2002). Chinese
Taoist cognitive psychotherapy in the treatment of generalized
anxiety disorder in contemporary China. Transcultural
Psychiatry, 39(1), 115–129. https://doi.org/10.1177/ 136346150203900105
.Link to the original article:
https://www.tandfonline.com/doi/full/10.1080/10503307.2023.2241626